Glass, Germs, and Steel:
Why Mayor De Blasio’s Draconian
Public Health Policy Will Fail
by Sarah Dillingham (May 2019)

A Family, Louis le Brocquy, 1951
Measles is in the news again. The humble microbe has many faces: scourge of the New World, benign and ubiquitous rite of childhood passage, simultaneous conduit of modern scientific achievement and vexing icon of evasive, unrealized dreamsculture war. U.S. measles cases spanning 22 states surged last month to 695 confirmed cases in 2019, marking the highest annual number since the disease was declared eliminated from the U.S. in 2000. The ongoing outbreak began last fall when infected travelers returned from Israel, Ukraine, and the Philippines, triggering clusters in New York, Washington State, and California—and a concurrent wave of proposed legislation to curtail non-medical exemptions for required childhood immunizations in over a dozen states.
As state legislatures considered bills tightening immunization requirements, U.S. Representative Adam Schiff formally requested censorship of vaccine-critical speech across social media platforms. The Congressional Committee on Health, Education, Labor and Pensions (HELP) also scheduled hearings designed to reinforce and amplify conventional wisdom blaming “vaccine hesitancy” for recurring outbreaks; witnesses were carefully selected to censure “anti-vaxxers” and quash safety concerns. That strategy was echoed in increasingly heated, polemical news reports and editorials condemning vaccine skepticism. This climate set the stage for two successive and unprecedented executive orders in Rockland County and Brooklyn, New York which sought to mandate vaccination under threat of criminal penalty for non-compliance. The trend culminated in President Trump—who has notably expressed concern over vaccine safety and considered spearheading a vaccine safety commission—urging citizens in no uncertain terms to “get the [Measles, Mumps, and Rubella] shot.”
Thus, measles and vaccine skepticism have captured our public consciousness as the cultural litmus test du jour, eclipsing such questions as whether Chief Justice Kavanaugh, the Covington students, and Jussie Smollett are villains or heroes, and which interpretation of events fits within a temperate and well-reasoned world view, versus that which constitutes “fake news.” Vaccine skeptics, at least those who openly define themselves as such, are too few in number to inhabit a significant voting block or define any major political party; and though state mandates are predominantly sponsored and passed by Democrats while a handful of libertarians and Republicans oppose them, the question of vaccine safety is traditionally non-partisan. Politicians and consumer advocates across the political spectrum increasingly find themselves relegated beyond the realm of the cultural mainstream when they voice even the most guarded criticism of the CDC-recommended vaccine schedule. National uptake of required vaccines for kindergarten-age children remains high, holding consistently above 90%. But if scientific studies are correct, those few dissenting public voices represent a much larger, silent swath of vaccine-hesitant health consumers: approximately 33–40% of parents delay or refuse one or more recommended vaccines, and those parents tend to be college-educated and disproportionately represented in STEM fields.
Read more in New English Review:
• Dysfunction Junction
• Jewtown: Poems of the Rise and Decline of Cork’s Jewish Community
• If TV’s So Good For You
Current legislation and predominant public opinion dictate that vaccine hesitancy or refusal is fundamentally unscientific, divorced from reality and—most importantly—deleterious to the public good. So what fuels this confounding, highly-educated third of U.S. parents who delay or refuse vaccines altogether? Are they solely responsible for thwarting the eradication of measles and other infectious diseases, as public health officials and editorial boards charge in unison? The recent measles outbreaks and resulting emergency orders to contain them provide a useful backdrop to examine this question.
Early last month, New York City Mayor Bill De Blasio declared a public health emergency as he unveiled an executive order mandating that “any person who lives, works, or resides” within four designated zip codes in the Williamsburg neighborhood of Brooklyn receive the Measles, Mumps, and Rubella (MMR) vaccine, or face criminal misdemeanor charges including $1,000 fines and imprisonment.
Williamsburg, an ethnically diverse neighborhood hosting one of the world’s largest Orthodox Jewish communities, is the epicenter of the current measles outbreak where 390 confirmed cases were reported as of April 24th (56% of reported U.S. cases), including 65 infants, 265 children aged 1 to 18 years, and 60 adults 19 or older—of which 83% are Williamsburg residents.
Flanked by Health Commissioner Oxiris Barbot and Deputy HHS Mayor Herminia Palacio, De Blasio outlined the details of the order in a 90-minute press conference, admonishing residents to “take measles seriously,” stating that “the only way to stop this outbreak is to ensure that those who have not been vaccinated get the vaccine.” The panel specifically addressed the Haredi community, singling out Orthodox Jews. “When the problem is overwhelmingly in one neighborhood, that gets people’s attention,” De Blasio noted. Strangely lacking was any mention of standard measures to control the spread of infectious disease—no discussion of hand washing, covering the mouth when coughing and sneezing, or quarantine at the first sign of illness. Instead the panel cited “anti-vaxxers spreading misinformation” and “received reports of so-called measles parties” as the cause of their failure to contain the outbreak during the previous months, despite aggressive outreach to secular and religious leaders and administration of 8,000 doses of MMR vaccine within an enclave of roughly 250,000 residents.
The announcement followed a similar emergency order unilaterally issued by Rockland County Executive Edwin Day on March 26th, which prohibited unvaccinated children 6 months to 17 years of age from all indoor public spaces. Representing several dozen Rockland parents, civil rights lawyer Michael Sussman successfully challenged the order on April 5th and won an appeal seven days later, arguing that four active cases throughout the county did not warrant an ongoing quarantine of healthy, unvaccinated children. In the wake of this precedent, Sussman announced plans to challenge the New York City order as well, charging that De Blasio and City health officials “overreached their authority” in mandating vaccination for all adults and children over six months of age with no option to self-quarantine. De Blasio repeatedly expressed confidence that his extraordinary action will withstand all legal challenges.
The first challenge to De Blasio’s order was filed the following week by New York attorney Robert Krakow, joined by attorney Patti Finn and Children’s Health Defense founder Robert F. Kennedy, Jr. The case was subsequently dismissed by Judge Lawrence Knipel, who found that the petitioners “failed to demonstrate entitlement” to the injunctive relief they sought, further stating “A fireman need not obtain the informed consent of the owner before extinguishing a house fire. Vaccination is known to extinguish the fire of contagion.” However the criminal misdemeanor penalty was quietly removed in a subsequent resolution issued by the Board of Health on April 17th.
In the weeks following these executive orders, reported cases in New York surged despite drastic measures to contain them. Why are these policies failing, and are “anti-vaxxers” with their “frank untruths” solely to blame? The pattern of this outbreak and the extreme draconian response beg some important questions; it behooves both architects and recipients of public health policy to consider them carefully.
Does the Emergency Order Serve Mayor De Blasio’s Stated Goals?
The goal of the Public Health Department in any emergency infectious outbreak is presumably to contain the spread of disease and mitigate the severity of illness in each case. City officials’ singular objective, as they describe it, is to get everyone vaccinated. In pursuit of this primary goal, they have effectively criminalized measles infection and lack of measles immunity—does this undermine the broader goal of containing the spread of measles?
Published New York state immunization data for school years 2013–2017 reflects that immunization rates for public and private schools in the cited Williamsburg zip codes was 96-97% those years. Only a handful of schools had vaccination rates lower than 90% (and of those, the lowest uptake was 83%); yet healthy, unvaccinated students were banned for many weeks from attending schools where there had not been a single case of measles, with no indication of when the ban would be lifted. Commissioner Barbot explicitly acknowledged that parents who participated in reported “measles parties” likely did so to obtain serologic proof of their children’s measles immunity (a positive measles antibody titer blood test) so the children could to return to school. Despite months of quarantining unvaccinated children from schools, the Williamsburg outbreak was not contained. Health Department policy inadvertently implemented a strong incentive for vaccine-hesitant residents to seek deliberate exposure to measles. Would it have been more effective to swiftly quarantine all susceptible children in schools where measles cases occurred, and allow all other children to remain in school?
It’s likely that quarantining unvaccinated school children failed to contain the outbreak because only 19% of reported cases occurred among children aged 5 to 18 attending grades K-12. Fully 32% occurred among adults and infants under one year old; quarantining children from schools and day care would not prevent contact among those groups. Further, if vaccinating one-third of the population failed to prevent these new cases, will the emergency order contain the outbreak? Conventional logic dictates that only unvaccinated people are infecting the new cases; however 11-22% of confirmed cases in Brooklyn are vaccinated. Are these vaccinated cases perhaps more likely to expose others because they and their healthcare providers don’t suspect measles during those critical four days when symptoms of illness and contagion begin, before the onset of the telltale rash?
Even if we accept the premise that compelling every unvaccinated person in Williamsburg to receive MMR vaccine will contain the outbreak, will the emergency order accomplish that goal? Officials are implementing the order via deployment of “disease detectives” in affected areas, who employ the technique of contact tracing to locate actively infected people and work outwards identifying every exposed community member. However, the order outlines that “a person with measles or an unvaccinated child exposed to measles in one of the above ZIP codes” is in violation and subject to civil penalties. Every good detective knows their informants cooperate solely on the basis of established trust and immunity from criminal prosecution; if fear and mistrust already hobbled the efforts of health officials to identify and contain potential cases, will criminalizing seronegative residents, deeming them a “public nuisance,” further drive these cases out of officials’ reach? Haredi Jews were already targets of unfounded fear and hostility before Mayor De Blasio publicly admonished their community, and his message may have intensified discrimination and mutual distrust among residents. Will the ultra-Orthodox residents of Williamsburg be forthcoming in fingering their friends, neighbors, and relatives to public health “detectives?”
Travelers in and out of Williamsburg have sparked new outbreaks in Michigan and Maryland. Will residents take refuge out of town if the directive continues? Have the Mayor and Health Commissioner undermined months of community relationship building by characterizing Williamsburg residents as “anti-vaxxers spreading misinformation and frank untruths” and criminalizing very personal religious beliefs and medical decisions?
The most effective containment policy, we might assume, would encourage residents possibly exposed to or infected with measles to identify themselves and their contacts without fear of retribution, and reward rather than penalize voluntary cooperation with public health officials. It would also define and directly address the “misinformation” which officials identify as a primary impediment to containment.
Is Measles a Mild or Severe and Dangerous Illness?
Drs. Barbot and Palacio repeatedly declined requests to explain the concerns and “misinformation” fueling vaccine hesitancy and alleged “measles parties.” Here is a concrete example of the paradox of dueling narratives: is measles a mild illness and standard rite of childhood passage, or is it a gravely dangerous disease which puts vulnerable citizens at risk? Is it possible that both could be true?
Addressing that question in sufficient detail to effectively discourage deliberate measles exposure would unveil underlying cracks in public health policy which officials seem loathe to confront directly. Instead the panel alluded to this paradox in vague terms, invoking “health dangers that are different than we’ve seen in the past,” and characterizing pre-vaccine era exposure parties as a popular way “to get the disease over with before children were late.”
What was the reality in the modern pre-vaccine era and why are health dangers different? Dr. Palacio attributed the difference to “medical advances” and “people living longer with severe medical conditions . . . who are on chemotherapy.” While 5-year survival rates may reflect either longer overall survival or earlier detection of cancer, Dr. Palacio failed to identify an important source of immunocompromised people today: the rapid rise of pediatric cancers in the U.S. There are currently proportionately more children with cancer in schools and day care centers than in 1963, when the measles vaccine was licensed. However, immunocompromised children are vulnerable to all infectious illnesses as well as exposure to recently vaccinated people. The MMR package insert confirms that vaccinees shed live-attenuated rubella virus for several weeks, and cancer center visitor guidelines—some of which were quietly archived after the Disneyland outbreak in 2015—nonetheless clearly articulate the current standing protocol: severely immunocompromised people must avoid contact with recent MMR recipients as well as exposure to measles, or the common cold, or other infections.
The primary population specifically at risk from measles exposure, in contrast to 1963, are infants under 6 months old for whom vaccination is neither safe nor effective, and who were protected by transplacental antibody transfer from immune mothers in the pre-vaccine era. However, these infants are at risk today because their vaccinated mothers are not conferring adequate or lasting transplacental antibody protection, as Dr. Barbot’s statement reflects: “The reality is that we have had children, younger than six months, exposed to the measles and have gotten the infection. So we want to prevent more of those cases.” These children would not have been at risk in 1963, when both infants and adults had robust protection from measles and deliberate exposure was therefore much safer than it is today. Deliberate exposure during the modern pre-vaccine era protected children from more serious disease in their teens and adulthood, and ensured the protection of their future infants.
Mortality rates from all infectious diseases, including measles, were high during the early 20th century when proper sanitation and nutrition were not universally available. However in the decade prior to 1963, there were 3-4 million measles cases annually with about 500,000 reported cases and 400-500 deaths per yeardescribed measles in 1962 as a “self-limiting infection of short duration, moderate severity, and low fatality.” Virtually all Americans contracted measles before the age of 15, and were immune throughout their lives. The several hundred annual deaths which occurred during that period were clustered primarily among children under the age of two, who were susceptible to measles and other infectious diseases because breastfeeding was discouraged—only about 15% of mothers breastfed their babies beyond three months. As acquired maternal immunity dissipates in infants aged 6-12 months, mothers with lasting natural immunity transfer antibodies and disease-fighting nutrients through their breastmilk. This protects infants and toddlers until weaning age, when measles and other childhood illnesses are typically mild with very few dangerous complications.
However by 1990, roughly half of all cases occurred in children under 5 years old with 17% among infants under 12 months old, and one-third of all cases occurring in patients over the age of 15. The mortality rate among reported cases was 3.2 per thousand, or 0.3%. Of 27,672 reported cases, 18% were vaccinated people, prompting the CDC to recommend a second dose of MMR for children aged 4-6. The hospitalization rate in the pre-vaccine era was 48,000 cases per year, or approximately 1.5% (10% of reported cases). In 1990 the hospitalization rate among reported cases had risen to 21%.
While measles was far less prevalent than it had been prior to mass vaccination, cases which did occur were striking age groups more susceptible to complications, thus rendering the disease more serious—particularly for unprotected infants. But articulating this difference begs another question: why don’t vaccinated mothers confer adequate protection to their infants?
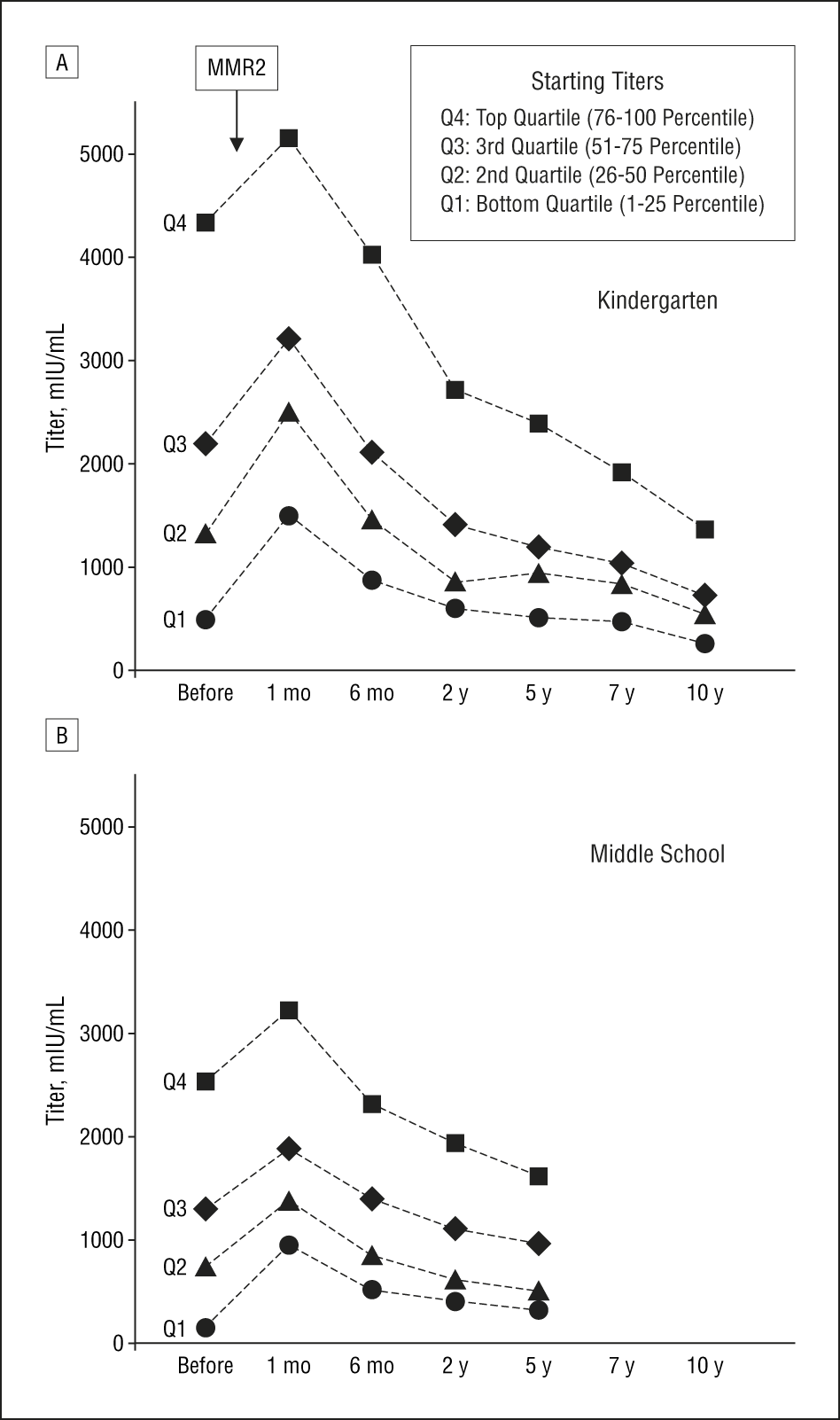
Public health officials frequently cite the 97% effectiveness rate of the two-dose MMR regimen—however this figure describes the 3% primary failure rate of the MMR, or the number of vaccinees who fail to initially develop antibody protection with their second dose. Vaccinees are also prone to secondary vaccine failure, or waning immunity over time. The 97% protection rate does not persist over time, as this 2007 study demonstrates: among recipients of 2 MMR doses, only the top quartile retained potent antibody protection after 5-10 years, while the bottom quartile were susceptible to full-blown clinical measles infection and the remaining 50% could develop subclinical, yet contagious modified measles. The authors concluded that 33% of 2-dose recipients were susceptible after 20 years, an interval which coincides with childbearing age for recipients who received their second dose at age 4-12.
{kind=link}
This phenomenon of waning immunity could explain why vaccinated mothers fail to confer effective antibody protection to their infants, and why babies under six months old are affected by current outbreaks. While public health officials accept documented proof of two MMR doses as “presumptive immunity,” one-third of fully vaccinated people are potentially susceptible to measles infection and transmission. Potential susceptibility among vaccinated people is reflected in the proportion of vaccinated cases in vaccine-era measles outbreaks:
| Measels Outbreak | >1 dose* | >2 doses** | Unvaccinated | Unknown | Total Cases | % Vaccinated |
| United States 1990 | 5,100 | — | 22,532 | 40 | 27,672 | 18-19% |
| United States (Disneyland) 2015** | 28 | — | 71 | 60 | 159 | 18-55% |
| Minneapolis, MN 2017 | 2 | 3 | 68 | 2 | 75 | 7-9% |
| Rockland County, NY 2018 | 10 | 6 | 162 | 23 | 201 | 8-19% |
| Brooklyn, NY 2008-19* | 43 | — | 304 | 43 | 390 | 11-22% |
| Clark County, WA 2018-19 | 3 | — | 63 | 7 | 73 | 4-14% |
*Number of doses received is undisclosed
**One case reported in California during the 2014-15 Disneyland outbreak received 3 doses of measles vaccine
Fully vaccinated people can contract and transmit measles, as demonstrated by recent outbreaks in which the index case was fully vaccinated, as well as outbreaks in fully vaccinated populations. In fact, vaccinated people whose immunity has waned and infants with little or no inherited immunity represent gaping holes in what was once robust, naturally acquired community immunity. These gaps in community protection may be at least as significant as small pockets of unvaccinated children and adults in contributing to current outbreaks, and in particular to the number of complications and hospitalizations among reported cases. They are an unintended consequence of the failure to completely eradicate measles within 1 year as forecasted in 1967 by Dr. Langmuir and his colleagues, who did not anticipate the ripple effect across decades of a mass vaccination program which was initially 93-97% effective but only 67% effective in the long term. In this way, mass vaccination of the entire susceptible population during the 1960’s was something like giving an individual subject an incomplete course of antibiotics. The wild measles outbreaks which persist are small in number, but more virulent than the mild, continuous background infection amid the susceptible childhood population in the pre-vaccine era.
Does Misinformation Fuel Vaccine Hesitancy?
Public health officials, legislators, and media outlets forcefully reiterate the general message that the MMR vaccine is “safe and effective.” However the “safety” of drugs and medical interventions is expressed in statistical terms: a drug or procedure which causes 1 death per 10,000 cases could be described as relatively “safe,” meaning theoretically safer than the immediate health problem the drug is employed to treat—although it was not safe for the subject who died after receiving it. Health officials weigh the relative risks of medical interventions against the risks of the conditions they treat; but this risk analysis is less straightforward for prophylactic interventions such as vaccines, which are administered to entire populations of healthy subjects. Vaccine hesitancy may be fueled by examination of the specific risks associated with the MMR, as opposed to gross misinformation.
Read more in New English Review:
• Houellebecq and the Popularity of the Crisis of Meaning
• Why Was Netanyahu Elected to an Unprecedented Fifth Term?
• The Monstrous Evil that is Sudan’s Bashir: Killing One-Third to Rule Two-Thirds
Specific MMR risks are difficult to weigh accurately against measles risks, as the relative risks of measles are ever-changing across different populations and conditions, and available safety data on the MMR may be incomplete. One Cochrane review of over 60 safety studies concluded that “the design and reporting of safety outcomes in MMR vaccine studies, both pre- and post-marketing, are largely inadequate.”
MMR vaccination is a subcutaneous infection with live-attenuated vaccine-strain measles, mumps, and rubella viruses. Although the attenuated vaccine-strain viruses are mutated to replicate slowly, subcutaneous injection bypasses the mucous membranes and cell-mediated immune response to infection; approximately 5-15% of vaccinees will develop a modified, non-communicable infection with symptoms which may include fever, rash, and presentation indistinguishable from clinical measles infection without tests to genotype the virus strain. (For instance, during the Disneyland measles outbreak of 2015, 194 cases were submitted for genotype testing of which 73 were vaccine-associated attenuated viral infections, and excluded from official counts of wild-strain measles cases.) Each person and each immune response is unique; and some of the same risks associated with measles infection are associated with the MMR.
The risk of febrile seizures from MMR may be anywhere from 0.03–0.16%, compared with a 0.03–0.65% risk from measles infection. Encephalitis is a documented risk of the MMR in some children, but the specific rate at which it occurs is not rigorously tracked. (The MMR package insert cites the risk of encephalitis/encephalopathy as 1 instance per 3 million doses, but references a single 1981 study which reports a rate of 1 instance per million recipients.) The comparative encephalitis risk from measles may be 0.005–0.1%. Subacute sclerosing panencephalitis (SSPE), a rare but devastating and fatal measles complication striking primarily those who were infected as infants, occurs after 5-10 per million measles infections and 1 per million MMR vaccinations. The MMR carries a 12-26% risk of arthralgia or arthritis in post-pubertal female vaccinees, a 0.003% risk of idiopathic thrombocytopaenic purpura (ITP) —a temporary but potentially dangerous condition causing low platelet count, and 1.8-14.4 anaphylactic reactions per million doses. The MMR package insert states that risks of cancer, genetic mutation, and impaired fertility have never been studied.
The MMR insert lists death as an adverse event, but does not disclose the mortality rate. The only MMR-associated mortality data available to the public is captured in the Vaccine Adverse Events Reporting System (VAERS), a passive reporting system created and co-managed by the CDC and FDA. Both the FDA and an independent 2010 Harvard University review found that VAERS may capture fewer than 1% of adverse reactions, and VAERS entries are not rigorously screened for consistency or accuracy. Given these caveats, it’s difficult to evaluate the 462 deaths associated with measles vaccine reported in VAERS and place them into context with the 0.01% measles mortality rate discussed above. The only other publicly managed source of injury statistics is the National Vaccine Injury Compensation Program, established in 1986 to indemnify vaccine manufacturers against lawsuits while compensating the families of injury victims. A 1998 formal review of NVICP claims identified 8 deaths associated with measles vaccine.
Vaccine-hesitant parents may also consider their ability to actively reduce or eliminate the risk of measles complications with proper medical care and sufficient Vitamin A, both before exposure and during infection. And while the risks of measles infection are closely monitored and well documented, the potential risks of MMR vaccination are largely unknown. Is it really fair or reasonable to characterize documented risks associated with vaccination as “misinformation” or those who consider them “anti-vaxxers?”
Mayor De Blasio and Commissioner Barbot dismissed citizens’ religious objections out of hand, declaring that “the religious leaders that we have met with have made it clear that there is nothing in Talmudic Law that prohibits vaccination.” The Washington Post echoed this assertion two days later, characterizing vaccine refusal as “a decision not based on any religious proscription.” However Orthodox rabbis are by no means unanimous in their relative endorsement or rejection of routine vaccination. Rabbi William Handler, a Holocaust survivor, explained the proscriptions directly to Assemblyman Jeffrey Dinowitz in an impromptu meeting with about 60 disgruntled constituents.
Public health officials, journalists, and others outside the Orthodox community may misunderstand the Halachic principle of Pikuach Nefesh— “to save a life” —which allows violation of religious commandments if life-saving medications are needed, or someone must ride in an ambulance on the Sabbath, and so forth. Vaccines containing WI-38 human diploid lung fibroblasts obtained from aborted fetal tissue and fetal bovine serum could certainly conflict with kosher law; so the question becomes whether the MMR vaccine, a prophylactic non-emergent intervention, will save more lives than it costs. This fundamental question directly mirrors the secular debate which informs vaccine hesitancy on secular philosophical and medical grounds. Rigorous debate over the meaning and proper application of Talmudic text is a fundamental cornerstone of Orthodox Jewish tradition; is it legal or morally defensible to criminalize this dialogue? Do Mayor De Blasio and public health officials serve their goal of containing the measles outbreak by publicly disparaging these religious and secular discussions?
Last week, Mayor De Blasio announced his plans for a proposed ban on steel and glass structures in the interest of reducing global warming. Curbing carbon emissions, like containing the spread of measles, is a laudable goal. Sadly, it’s often the very worthiness of an endeavor which inspires the most misguided policies and imprudent vehemence in their application. Commissioner Barbot asserted that “it is important that all New Yorkers get vaccinated.” If the Williamsburg emergency order failed to contain the outbreak and Mayor De Blasio were to extend the mandate to all 8.6 million New York City residents, he would potentially be mandating up to 1.3 million attenuated viral infections, 258,000-1.4 million febrile seizures, 258 cases of ITP, 8 fatal cases of SSPE, 8 potentially fatal allergic reactions, and an unknowable, unquantifiable number of deaths—among residents who may have preferred the 0.2% chance of encountering a fellow citizen infected with measles if properly informed. And among those fully vaccinated New Yorkers, one-third would potentially be susceptible to measles infection again as their immunity waned.
A more temperate and effective approach might include instructing residents to consume adequate vitamin A with the guidance of a physician, and self-quarantine at the first signs of infection; encouraging cooperation with public health officials without threat of retribution; and explaining clearly why deliberate exposure endangers infants and vulnerable adults in the vaccine era. When guided with relevant information and adequate options for cooperation rather than coercion, citizens do the right thing.
«Previous Article Table of Contents Next Article»
__________________________________
Sarah Dillingham is a freelance writer on matters of health and wellness, and mom to a rambunctious boy in the D.C. suburbs.
Follow NER on Twitter @NERIconoclast